
Opening/Background:
Hypermobile type Ehlers-Danlos Syndrome (hEDS) is a rare inherited disorder involving connective tissues, often characterized by skin hyper flexibility and fragility, increased scarring, and bruising, delayed wound healing1-3. One of the most notable signs however is the presence of hypermobile joints3-6, including the temporomandibular joint (TMJ). In most cases of generalized hypermobility disorders, such as hEDS, pain is not associated with degeneration of the discs rather the weakness of the connective tissue ligaments supporting the TMJ structure7. Painful or mechanically inhibited jaw opening is correlated to the degree or severity of hEDS and associated weakness of ligaments8-10. The diagnosis and treatment of these cases are complex and often require orthognathic surgery to reposition the mandible and subsequently the TMJ.
A multidisciplinary approach including prosthodontic consultation prior to any treatment is crucial to the success and outcome of the case11. A prosthodontist can improve the outcomes of maxillofacial involved cases through proper determination of the appropriate vertical dimension of occlusion (VDO), determining the proper implant placement locations, esthetic determination as well as proposing the potential achievable treatment outcomes12-15.
Clinical Report:
A 29-year-old partially edentulous female patient with significant medical history including hEDS, congenital ankylosis of both TMJ, chronic neuropathic pain and previous attempts at complete TMJ reconstruction presented to the Harvard School of Dental Medicine, Boston, MA. Her chief complaint being, “I want to be able to chew and smile again”.
The patient endured two previous TMJ reconstruction attempts, each providing various issues over time. Due to multiple attempts at placing a permanent TMJ prosthesis, excessive amounts of soft tissue scarring was noted and contributing to limited opening. As a result, the patient displayed chronic poor hygiene and caries due to limited access, pain on brushing and a near lack of dental follow-up (Fig. 1). The patient was seen by prosthodontics for a ‘hand-and-mirror’ exam one day prior to full mouth extractions. The patient opted for full mouth extractions due to caries and consistent odontogenic pain. Prosthodontics determined the maxillary cuspids (#6 and #11) should remain since periodontally probing depths ranged from 1- 3mm and caries present were not excessive in depth. Following this prosthodontic consultation, the patient had the remaining dentition extracted excluding #6 and #11.
Two months later, the full prosthodontic evaluation revealed severely limited opening with an inter arch maximum distance of around 18mm (from alveolar ridge to ridge) (Fig. 2A and 2B). The maxillary tuberosities were 2mm superior to the retromolar pads bilaterally. The goal of maintaining the cuspids served as a reference during the mandibular repositioning and subsequent use as a potential abutment for future overdenture treatment.
Stock edentulous upper and lower impression trays were extensively modified to fit the patient without pain and excessive pressure on the TMJ. For the maxillary tray, relief holes were drilled in the area of #6 and #11 to allow for passive seating of the tray for more intimate contact with the soft tissues. Trays were border molded with modeling plastic impression compound (Green Wax Impression Compound Stick; Kerr Corp). The impression was taken (3M™ ESPE™ Impregum™ Penta™ Polyether Impression Material). The impression material was wiped from the cuspids prior to setting. The teeth were captured in the same impression with a heavy bodied puddy pickup after the initial soft tissue impression was completed. The lower impression was taken with traditional border molding and impression steps. The impressions were poured with type 3 gypsum stone.
An open bite was taken. Heavy bodied puddy was mixed and rolled into a horseshoe shape and placed on the maxillary arch to key into the cuspids. Bite registration material was used on the base of the patty and the patient was instructed to lightly bite into the material (~1mm). The maxillary portion of the bite registration patty now cut back to have no hard or soft tissue contact. The patty was placed on the lower arch, and bite registration material was placed on the maxillary portion of the patty and the patient was instructed to lightly bite into the material (~1mm) (Fig. 3). A facebow record was obtained. Casts were mounted on and ARTEX (add full name).
A mandibular repositioning device was fabricated utilizing wax at the increased VDO. The pin was raised to +9mm to allow for proper posterior freeway space (Fig. 4). The wax prosthesis included three soft tissue holding areas and two hard tissue teeth key areas. No try in was possible due to the patient’s limited opening. The wax prosthesis was processed into clear acrylic PMMA with the Ivobase system. Excess material was removed and the prosthesis was polished to a shine to allow for proper visualization of seating during the surgery (Fig. 5).
Discussion:
In most TMJ reconstruction cases, the teeth are often utilized as a reference in positioning the mandible16. Difficulties arise when these reference points, such as the teeth, are missing. In this case, traditional border molding and impression taking were similar to traditional conventional denture fabrication. The difficulties arise from the wax-rim step, as traditional conventional methods will not work. Due to the limited opening, wax-rims with the largely accepted 18mm posterior height would not fit in the patients mouth, thus an open mouth bite registration was used for a rough arch position estimate.
It was determined to increase the vertical around 9mm as the position would allow for enough room prosthetically for complete dentures as a final restorative treatment. In this case, with the previous history of TMJ reconstruction attempts and amount of scar tissue, only rotational movement was possible. A discussion was had to move the mandible in an inferior and anterior movement yet was determined not possible by the surgical team. The mandible was opened in a position displaying only a rotational movement as a result.
Summary:
This clinical report discussed a method of mandibular repositioning of an edentulous ridge not otherwise available in the literature.
Figures:

Figure 1: Panoramic radiograph of the initial patient presentation to the oral surgery department.


Figure 2A: Intraoral photo at the time of the prosthodontic consultation. (have a few other pictures to choose from)

Figure 2B: Intraoral photo at the patients maximum mouth opening
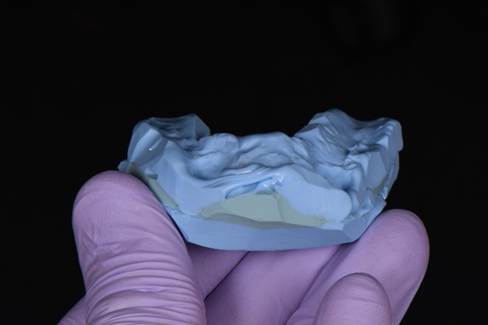
Figure 3: Sequential bite registration




Figure 4: Wax mandibular repositioning device at an open vertical dimension



Figure 5: Processed clear PMMA acrylic surgical positioning stent
References:
- Malfait F, Wenstrup RJ, De Paepe A. Clinical and genetic aspects of Ehlers-Danlos syndrome, classic type. Genet Med. 2010 Oct;12(10):597-605. doi: 10.1097/GIM.0b013e3181eed412. PMID: 20847697.
- Parapia LA, Jackson C. Ehlers-Danlos syndrome–a historical review. Br J Haematol. 2008 Apr;141(1):32-5. doi: 10.1111/j.1365-2141.2008.06994.x. PMID: 18324963.
- Lepperdinger U, Zschocke J, Kapferer-Seebacher I. Oral manifestations of Ehlers-Danlos syndromes. Am J Med Genet C Semin Med Genet. 2021 Dec;187(4):520-526. doi: 10.1002/ajmg.c.31941. Epub 2021 Nov 6. PMID: 34741498; PMCID: PMC9298068.
- Mitakides JE. The effect of Ehlers-Danlos syndromes on TMJ function and craniofacial pain. Cranio. 2018 Mar;36(2):71-72. doi: 10.1080/08869634.2018.1435092. PMID: 29480137.
- Mitakides J, Tinkle BT. Oral and mandibular manifestations in the Ehlers-Danlos syndromes. Am J Med Genet C Semin Med Genet. 2017 Mar;175(1):220-225. doi: 10.1002/ajmg.c.31541. Epub 2017 Feb 13. PMID: 28192626.
- Castori M, Morlino S, Ghibellini G, Celletti C, Camerota F, Grammatico P. Connective tissue, Ehlers-Danlos syndrome(s), and head and cervical pain. Am J Med Genet C Semin Med Genet. 2015 Mar;169C(1):84-96. doi: 10.1002/ajmg.c.31426. Epub 2015 Feb 5. PMID: 25655119.
- Chang TH, Yuh DY, Wu YT, Cheng WC, Lin FG, Shieh YS, Fu E, Huang RY. The association between temporomandibular disorders and joint hypermobility syndrome: a nationwide population-based study. Clin Oral Investig. 2015 Nov;19(8):2123-32. doi: 10.1007/s00784-015-1422-7. Epub 2015 Feb 17. PMID: 25687768.
- Baeza-Velasco C, Van den Bossche T, Grossin D, Hamonet C. Difficulty eating and significant weight loss in joint hypermobility syndrome/Ehlers-Danlos syndrome, hypermobility type. Eat Weight Disord. 2016 Jun;21(2):175-83. doi: 10.1007/s40519-015-0232-x. Epub 2015 Oct 27. PMID: 26506923.
- Willich L, Bohner L, Köppe J, Jackowski J, Hanisch M, Oelerich O. Prevalence and quality of temporomandibular disorders, chronic pain and psychological distress in patients with classical and hypermobile Ehlers-Danlos syndrome: an exploratory study. Orphanet J Rare Dis. 2023 Sep 19;18(1):294. doi: 10.1186/s13023-023-02877-1. PMID: 37726791; PMCID: PMC10510186.
- Cohen A, Sela MC, Ran LZ, Rushinek H, Talisman S, Casap N. Increased Prevalence of Generalized Joint Hypermobility Observed in Patients With Recurrent Temporomandibular Joint Dislocation. J Oral Maxillofac Surg. 2023 Aug;81(8):950-955. doi: 10.1016/j.joms.2023.04.006. Epub 2023 Apr 20. PMID: 37160256.
- Rechtin M, Krishnan DG. A Decade of Complications Following Total Temporomandibular Joint Reconstruction (TJR) in a Patient with Ehlers-Danlos Syndrome. Another Surgical Misadventure or An Absolute Contraindication for TJR? J Oral Maxillofac Surg. 2021 Oct;79(10):2059.e1-2059.e5. doi: 10.1016/j.joms.2021.05.016. Epub 2021 May 19. PMID: 34153263.
- Lechner SK, Champion H, Tong TK. Complete denture problem solving: a survey. Aust Dent J. 1995 Dec;40(6):377-80. doi: 10.1111/j.1834-7819.1995.tb04836.x. PMID: 8615743.
- Goldstein G, Goodacre C, MacGregor K. Occlusal Vertical Dimension: Best Evidence Consensus Statement. J Prosthodont. 2021 Apr;30(S1):12-19. doi: 10.1111/jopr.13315. PMID: 33783090.
- Narby B, Kronström M, Söderfeldt B, Palmqvist S. Prosthodontics and the patient: what is oral rehabilitation need? Conceptual analysis of need and demand for prosthodontic treatment. Part 1: a conceptual analysis. Int J Prosthodont. 2005 Jan-Feb;18(1):75-9. PMID: 15754898.
- Narby B. Factors shaping demand for prostethic dentistry treatment with special focus on implant dentistry. Swed Dent J Suppl. 2011;(218):3-65. PMID: 22338785.
- Krishnadas A, Subash P, Iyer S, Manju V, Thankappan K, Pullan S, Nerurkar SA, Vinay V. Controlling and Stabilising Mandible During Reconstruction: Significance and Techniques. J Maxillofac Oral Surg. 2023 Mar;22(Suppl 1):56-63. doi: 10.1007/s12663-023-01897-5. Epub 2023 Mar 22. PMID: 37041959; PMCID: PMC10082878.