
I don’t know about you, but I’ve really noticed my patients accepting, and even asking for dental implants to replace their missing teeth, lately. This is undoubtedly because dental implants in general today have enjoyed a good reputation as being a successful dental treatment alternative. It is thanks to all of the many outstanding continuing education courses taught today around the country for general dentists, not to mention dental school’s placing it into their curriculum, and AEGD/GPR’s training general dentists right out of school. Much to the chagrin of the oral surgery, periodontal and prosthodontic residencies programs, general dentists are no longer afraid to place dental implants in the general population of patients in the USA. This leaves the specialists with the most difficult of cases, as it should be.
I am not trying to say that I am an expert in placing dental implants. My oral surgeons and periodontists are still the gold standard for placing dental implants, and I will continue to refer those cases I do not feel comfortable doing myself. It is just that I find some dental implant cases relatively simple to do myself.
One type of case that was routinely referred out of my office was the dental implant verses the pneumatized sinus. I can remember back in dental school when my oral surgery instructors scared all the impressionable dental students with the sinus “black hole”. We were taught that one of the worst things in the world was to extract a tooth and break through the schneiderian membrane. Now we have instructors like Dr. Michael Pikos of Palm Harbor, Florida presenting to the ICOI (Vancouver) that it is not terribly bad to tear the membrane, and you can practically remove it all, and still do a sinus lift bone graft.
There are some implant cases that I have identified needing a sinus lift to place an implant that could be done by lifting the floor of the sinus through the osteotomy site a few millimeters. There are several methods for doing this procedure and I feel patients accept these lifts better that the lateral window (considering the cost and scope of procedure).
I will show you the one I’m using, it is called the Hatch Reamer. 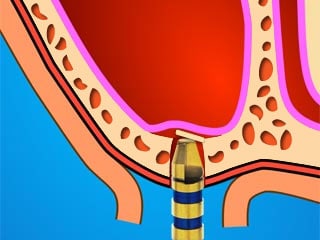 The name “Hatch” comes from what the bone looks like when the reamer penetrates through the sinus floor cortical bone.
The name “Hatch” comes from what the bone looks like when the reamer penetrates through the sinus floor cortical bone.
I went out to L.A. in 2008 to attend a hands-on workshop at a Periodontist’s office called Dr. Jin Kim. He showed us how to do a sinus lift with the Hatch Reamer while using PRP mixed into the bone grafting material.

Pictured above is a very simple kit of different sized “HatchReamers” and bone pluggers.
This is a look from inside the sinus of a Hatch Reamer sinus lift.
Case #1
This is a case of a 51 y/o/w/f who had orthognathic surgery for skeletal class 2 malocclusion back in her twenties. The surgeon took out the first premolars and removed that bone to make up for her excessive maxilla. Some thirty years later she began to have sensitivity on #4 and the following x-ray was take as a part of a FMX.

The periapical area for tooth #4 was unremarkable, but the mesial cervical looked suspicious. At first it looked like root caries on the mesial of #4, but after elevating a flap it was found to be external resorbsion. She didn’t want to loose the tooth. Treatment plan: Endo/post/crown with crown lengthening.

Told her the prognosis was guarded because bone had begun to invade the side of her tooth and that the canine (#6) was beginning to show signs of the same resorbsion, too. She was not interested in treating #6 at that time because everything felt much better after treating #4.

One year later, #4 is begining to bother her again. The tooth was extracted. Still she did not want anything done on #6.

Ten months later and now #6 is bothering her. Bone had invaded #6 distal. Treatment plan: Extract #6/bone graft #4, #6 and add #6 to transitional partial denture/heal for 6 months/implant/crowns #4, #6 with Hatch Reamer sinus lift.

Five months after extraction of #6 and bone grafting with Dynoblast/BioMend Extend collagen membrane: The sinus is too low in this area for long enough implants, so the sinus will be lifted through the osteotomy.
Actual patient chart surgery notes below: (Carestream/Kodak PracticeWorks)
Informed Consent signed, Reviewed health history, Sterile Field Established, Skin/Mouth Prep-betadine & peridex, surgical guide used, Elevated full thickness flap, sterile saline, Hatch Reamer to lift sinus through osteotomy, bone graft with Puros Allograft (cancellous 0.25-1mm), Zimmer Tapered Screw-vent 4.1mm X 13mm in #6 area, Type 3 bone, and Zimmer Tapered Screw-vent 4.1mm X 11.5mm in #5 area, Type 3 bone, bone level implant cover screws, decorticated facial cortical plate over #6-#4 and placed Dynoblast/BioMend membrane, 5.0 black silk suture, relieved F/ heavily so it would not move bone graft, Post-op Pano, Oral Hygiene Instructions, Topical anesthetic 20% lido/4% Tetra/2% phenylephrine with 3 carpules (108mg/5.1ml) of 2% Mepivacaine/1:20,000 NeoCobefrin infiltration, Pt informed not to eat food, bite or chew on lips or tongue while anesthetic is still working. Next Visit: Suture removal in 1 week and Second stage implant exposure in 5 months

Post-op panoramic showing ballooned up bone over the apices of #4 and #6 implants.
 5 months post-op with bone growing over the apices of the implants. (Sorry about the phosphorus plate artifact)
5 months post-op with bone growing over the apices of the implants. (Sorry about the phosphorus plate artifact)
6 month later, look what showed up on the opposite canine

This tooth was extracted, bone grafted and later replaced with an implant/crown without a Hatch Reamer sinus lift, (Astra Tech OsseoSpeed 3.5S X 11mm in #11 area, Type 2 bone).

12 months post-op CBCT

#4 CBCT

#6 CBCT
12 months later we purchased a CBCT and took pictures of #4-6 areas of the mouth.
This is in my opinion a good way to lift a sinus without a lateral window sinus lift bone graft. I am more than sure there are other ways to do sinus lifts with different instrumentation/techniques. This one is fast, easy and reusable. I recommend it to the beginner dentist who needs to get just a few more millimeters of bone to place an implant in the sinus area.
Other cases to come…