
This 61 y/o/w/f has been a long time patient at our office. She has become more incoherent over the past few years and is under psychiatric care. She made an appointment at our office for a loose tooth after an emergency room visit, but no showed. A week later she presents to our office looking like this:

She had fallen down and cut her upper lip and subluxated her maxillary right central incisor (#8). The following are notes cut and pasted out of her chart.
Day One:
EMERGENCY EXAM NOTE:
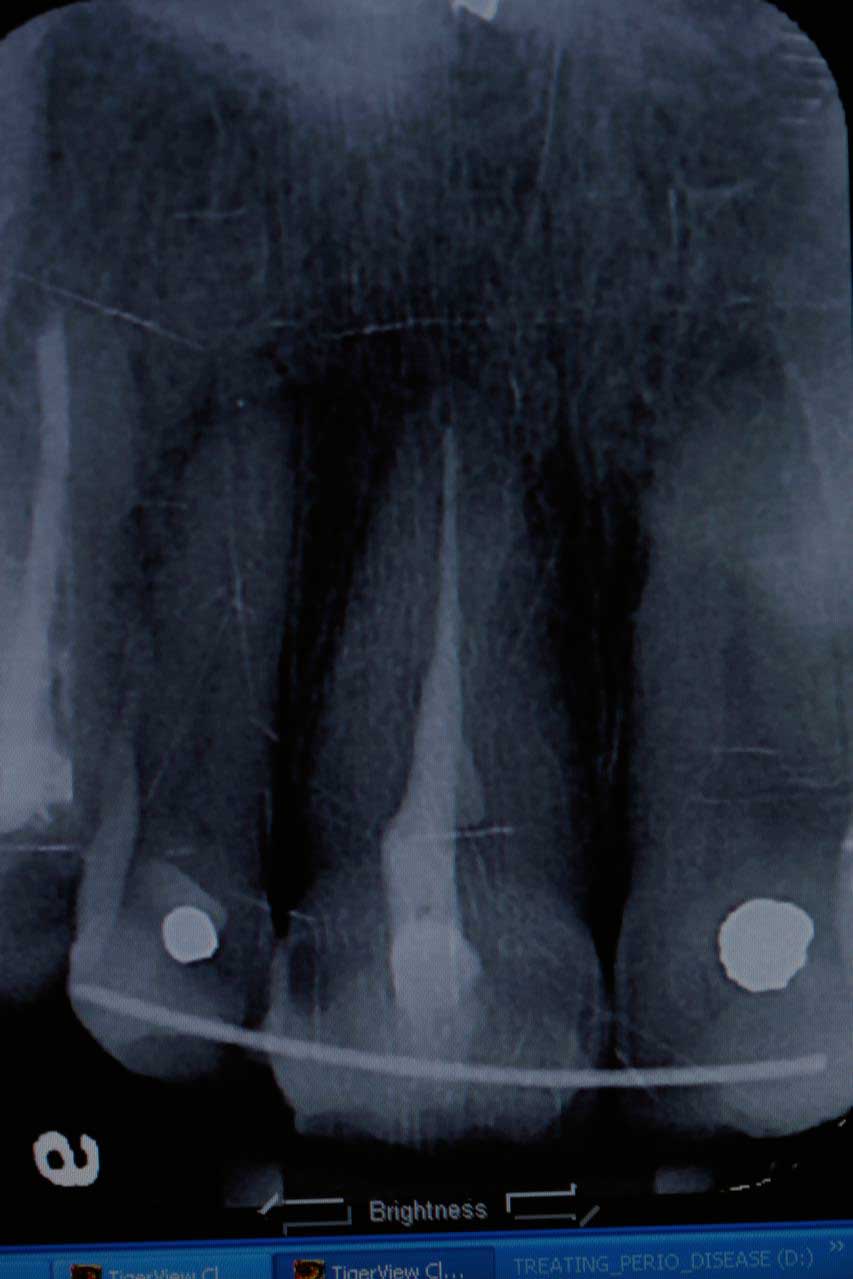
Periapical x-ray(#8) taken today by Laura with a lead apron and was reviewed by Dr. Mark Kraver.
SUBJECTIVE:
Reviewed health history, Chief complaints include points to tooth #8 that was almost knocked out 9 days ago and the patient didn’t see us that day even though she had an appointment.
OBJECTIVE:
Clinical and radiographic findings included #8 subluxated half out of the socket, still has sutures in the upper lip lacerations from the ER, TMJ appears normal, Oral Cancer screening WNL, the patient seems confused and rambled on about all kinds of other subjects mostly about her family matters.
ASSESSMENT: Not really sure if she can make a decission for her own treatment (she is here alone). At this point she can either have the tooth pushed back in and splinted with follow-up endo/filling or extraction and implant/flipper/crown.
PLAN: Photos, Re-implantation with it splint bonded and re-eval for endo VS extraction in 1 week.
Risks, benefits and alternatives have been discussed, Treatment plan accepted.


TREATMENT NOTE:
The tooth was hanging half-way out of socket. The trauma happened over a week ago. Firmly forced the tooth back into the socket and bonded it into place with a rectangular ortho wire (18X22) with H2O2/etch/PQ1/flowable/Filled composite to adjacent teeth. The patient has class 2 overjet. 1.7cc 4% articaine with 1:20000 neo. Photos. Soft diet. NV re-eval in 1 week for Endo.
Amoxicillin 500 mg
Disp 30 (thirty) Tabs
Sig. 2 tabs now & 1 tab q8hr until gone

One week Recall
TREATMENT NOTE:
Tooth healing well, photos, no discomfort, Informed Consent, Reviewed health history, Root Canal Treatment using Rubber Dam, Endo gripper, Apex Locator, necrotic pulp noted, File-Eze EDTA canal prep, Water irrigation, Er:YAG with eye protection, Photon induced photo-acoustic streaming (PIPS) 400u/14.0mm laser tip, (R14, 50us, 20mJ, 15Hz, 0.3W), EDTA, Water irrigation, #45 file @ 23.0mm, Periapical (2), resin coated GP w/ EndoRez, Cavit, Treatment was tolerated well. Topical anesthetic 20% lido/4% Tetra/2% phenylephrine with 1 carpule (36mg/1.7ml) of 2% Mepivacaine/1:20,000 NeoCobefrin (Onset/ 2 pain rating) infiltration, Pt informed not to eat hard foods. Do not bite or chew on lips or tongue while anesthetic is still working. Next Visit: Re-eval in 2 weeks, Filling(#8 L) and remove wire splint.
The patient has been informed that a final restoration will be needed. If this final restoration is not done in a timely manner then the tooth may be lost from possible recurrent decay, endodontic leakage, and /or fracture. Soft diet.
Two week Re-eval
TREATMENT NOTE:
Informed Consent, Reviewed health history, photos, Restoration was performed with Hydrogen Peroxide, Acid Etch, PQ1, DenMat Virtuoso Flowable, Filteck Supreme Plus, Composite Shade C3, Repair Endo Access, removed splint, photos, Treatment was tolerated well. Heavy plaque noted, Oral Hygiene Instructions (soft foods for 6 weeks), no anesthesia used, Next Visit: Re-eval, Recall


Two weeks later
PROPHY APPOINTMENT:
Refused doctors exam c/o already had exam this year, Prophylactic cleaning was done on the entire mouth, Oral Cancer screening WNL, Reviewed health history, recent lip trauma and sublimated #8, ProphyJet, Hand scalers, Treatment was tolerated well. Very ineffective OH, Heavy plaque noted, Moderate Stain, Oral Hygiene Instructions, Next Visit: 3 month recall.
The patient understands that this treatment is not intended to treat active or chronic periodontal disease (deep pockets).
Patient’s age is 61 and risk factors include: Poor oral hygiene, Many multi-surface restorations,
According to the above factors, I place this patient at this time in the High Risk Category and recommend Fluoride treatment. Informed of $20 fee for fluoride, fluoride varnish placed.
Discussed with the patient about adding xylitol to the patient’s diet to help control dental caries. Told that it has been shown that using 6.5 grams of xylitol daily for 2 months can help decreased dental caries. Xylitol along with daily fluoride rinses can help remineralize incipient tooth decay. She were give a sample packet of xylitol sugar and told to use it in cooking, after each meal and before bed.


The tooth was adjusted on the incisal edge for esthetic purposes and is a stable class 1 mobility after 3 months post-op. The patient has not improved her general health or oral hygiene. She still comes in for her routine dental cleanings.
The point that should be taken from this is that you can still treat partially avulsed teeth many days after the original trauma with the standard care used to treat completely avulsed teeth.
6 Month Recall

